

Nowadays there seems to be a pharmaceutical solution for all that ails you. Does your nose tickle? Pop this pill and fear tickles no more. Have an opiate problem? No problem, take this medication in the privacy of your own home. Only you and your doctor need to know. (Side effects may include: stuttering, nose bleeds, and sudden bouts of irrational behavior). Side effects from the medication? We have that covered too. Keep taking it, and here is another medication for constipation, another for restless legs, and yep, we even have something for waking up and falling asleep. Easy-peasy. Your addiction is now in control. Your monthly total from the pharmacy is a mere $843.24 and your Provider will be happy to continue this regimen for your “health,” as long as you continue to pay your bill.
This scenario may sound extreme, but it is a reality for many who are suffering from opiate addiction. This trend is steadily on the rise because we have an opiate crisis that has wreaked havoc on our country contributing to an increasing amount of overdose deaths yearly. Thankfully, the U.S. is scrambling to find solutions which are laid out in this press release by the U.S. Dept. of Health and Human Services and by the Five-Point Opioid Strategy that is currently being funded. This is a remarkable step in a positive direction for those suffering from opiate addiction, the families and loved ones of these people, and a huge step forward in lessening stigma and spreading awareness. But, we are not out of the proverbial woods yet. There are serious risks with one of the solutions being promoted, and, these risks are not yet being adequately addressed if we are to make actual progress towards helping the opiate crisis, saving lives and tempering a disease that affects our society as a whole.
The problematic strategy I am alluding to is Medicated Assisted Treatment (M.A.T.) which is explained here in detail by S.A.M.H.S.A. Research supports this as an effective way to help people stop using illicit opiates, insurance companies often pay for these medications in part, and treatment facilities are quickly adding M.A.T. to the treatment plans of clients with Opiate Use Disorder. For some, this is a great option, but is it good for all opiate addicts? And, are we on the verge of a “cookie cutter” intervention that could end up hurting more people than it is saving?
Medications being prescribed for M.A.T. protocols that pose potential cross-addiction problems are Methadone, Suboxone and Subutex. Originally, methadone and buprenorphine were used in harm reduction models (for people who have had multiple failed attempts at recovery and accept being on these medications long-term in an attempt lessen risk of illegal activities to acquire their illicit substances, for the addict to be able to maintain employment by not worrying about becoming ill from withdrawal symptoms so frequently, and, for less need to use needles and spread diseases). These are all great reasons to provide M.A.T., but, with the escalation of the opiate crisis, these primary reasons to offer these medications have shifted from a last resort treatment option to the first line of defense.

The problem is, these substances are in fact addictive as well, and, work on some of the same the opiate receptors in the brain that the illicit opiates work on. Filling these same opiate receptors is, in part, why they are being prescribed. This interaction helps stave off cravings and withdrawal symptoms, and, due to their longer half-life, the addict needs to use them less frequently than they needed to use the illicit opiates. However, having cravings and learning to walk through them using recovery tools is the basic nature of recovery from addiction and simply taking medication to avoid cravings does not provide this tool.
M.A.T. prescribing guidelines do suggest cognitive, behavioral, supportive therapies and applications as seen by the ASAM National Practice Guideline, which states: “At a minimum, psychosocial treatment should include the following: psychosocial needs assessment, supportive counseling, links to existing family supports, and referrals to community services.” But is this recommendation actually happening? Are Providers being held accountable for making sure clients are also seeking and receiving these therapies? I fear the answer is often, no.
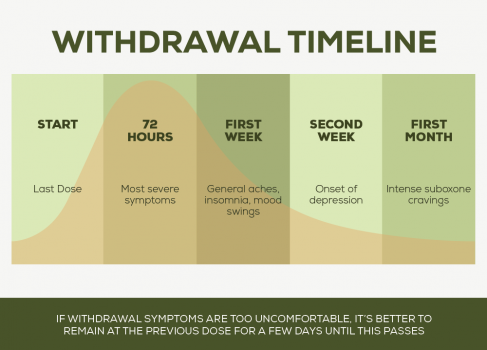
Another concern is that it is rarely discussed is that getting off of these opiate replacement medications is a long, expensive and painful process comparable to regular heroin or opiate withdrawal, but, with a much longer duration of withdrawal symptoms (due to the longer half-life that they are in fact prescribed because of). What is crucial to examine and address, is how can these people on M.A.T. be effectively helped to get off the prescribed M.A.T. medications and not revert back to their usual drug of choice especially in a “feetox” (a term coined by patients on methadone clinics who are being rapidly tapered down in dosage due to their inability to pay) situation. The most dangerous time for an overdose is when an addict has not used in a long time and reintroduces drugs into their system.
Isn’t this what we, as a society, are trying to avoid? I suggest more plans for support and help at the end of the medication tapers, more accountability that the person being tapered is getting help adjusting to a substance-free life and extra support during the detox/withdrawal symptom time period. Might this be the best time for inpatient, IOP or PHP levels of care and treatment? Should groups be designed specifically for this time period? And, isn’t this identical to opiate addiction treatment plans? It is, because this is the same problem— just a different substance.
Lastly, how can M.A.T. be overseen and monitored in terms of ethical practices because due to the longer length of this treatment modality it is also a potential cash cow for financial stakeholders? Addicts on maintenance programs are “billable” for much longer periods of time which unfortunately can, and has been taken advantage of by unscrupulous treatment centers and providers. M.A.T. medications are expensive, as are the medications for side effects. Is Big Pharma cashing in, once again, on addiction and people who are suffering and are in a compromised state? It is sadly quite possible and we have seen this before in our recent history with Purdue Pharma and their misinformation about addiction and their medication Oxycontin. The similarities are alarming.

Thank goodness we as a society are seeking solutions for the opiate crisis but let us not allow our compromised position of fear hastily push us into feeding the disease of addiction and possibly creating a future of more people addicted to even more substances. Let us not lose sight of the fact that recovery is possible, and, has been possible for millions of people for many decades by way of free support systems via recovery fellowships, by learning coping skills and techniques that focus on abstinence and living skills, and, by therapeutic modalities that address underlying issues that have led some to addiction. It is beautiful that our country has become more openminded and willing to find solutions for the opiate crisis. Continuing on this path, can we please explore more ways to help people find freedom from active addiction carefully, effectively and ethically without risking perpetuating the problem.




{kind=link}